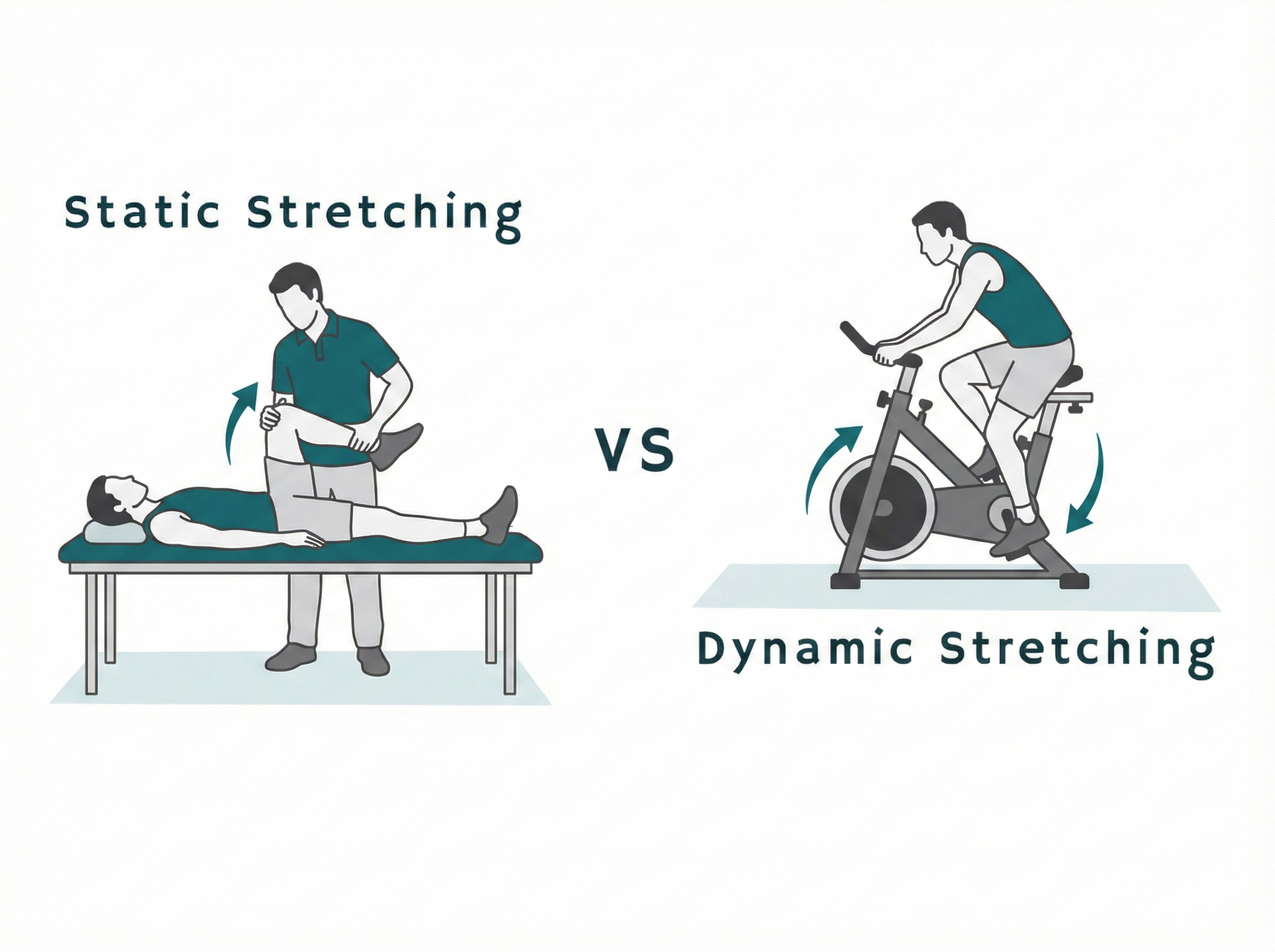
In the first two posts of this series, I explained what knee arthrofibrosis is and how dynamic stretching through controlled cycling works differently than traditional static stretching.
Post 1: Dynamic Stretching Below 60 Flexion: The Science of a Cycling Alternative for Knee Arthrofibrosis
Post 2: How Cycling with OrthoBike Stretches Knees with Arthrofibrosis
I suggest starting there.
In this post, I compare OrthoBike dynamic stretching (based on thirteen years of patients using OrthoBike as they rehab their joints) with a static stretching protocol recommended for arthrofibrotic knees: low-load prolonged stretching (LLPS). This post is not meant as a scientific paper.
What is Low-load Prolonged Stretching (LLPS)?
Low-load prolonged stretching (LLPS) is a form of static stretching (→ Post 2, "How Cycling with OrthoBike Stretches Knees with Arthrofibrosis") used in knee rehabilitation. The knee is moved into a stretch position and held there for an extended period of time using a brace or splint.
The “low-load” part means the force applied is not aggressive. The “prolonged” part means the stretch is held for hours at a time, often three to eight hours per day.
Comparing the benefits of OrthoBike cycling vs LLPS
The world of early stretching rehab changes when dynamic stretching through cycling therapy can be extended to rehabilitate knees with limited flexion.
Here is a benefits comparison between OrthoBike and LLPS.
Which benefit is most important to you?
1. Functional movement for daily life
How the two approaches translate into real-life function.
| OrthoBike (Dynamic Stretching) | LLPS (Static Stretching) |
|
Familiar movement, rest-of-life application, moving and strengthening both legs, repetitive motion. |
unfamiliar, short term, one leg immobile in the stretch position, other leg also immobile. |
| Resisted forward and backward pedaling for neuromuscular therapy, strengthening, extension therapy, pain-free. | Unidirectional and one-dimensional cranking on the knee; could be painful. |
| Walking and stairs: best exercise for regaining natural gait and speed, balance, complex motion. | You are immobile, does not translate into gait speed and balance. |
2. Effective knee therapy
How the efficacy of the two methods compares.
| OrthoBike (Dynamic Stretching) | LLPS (Static Stretching) |
|
Works extension and flexion at the same time, from the beginning of rehab. |
One-dimensional, flexion and extension are separate long-term therapies. |
| Warm up knee before stretching, then adjust for stretching. | No repetitive motion for warming up. |
| Limits stretching to mechanically controlled increments of flexion. | Gives incremental increases in loading with flexion angle estimates. |
3. Confidence and encouragement
How the two methods affect patient motivation.
| OrthoBike (Dynamic Stretching) | LLPS (Static Stretching) |
|
Encouraged by knowing where you are on therapy journey, thanks to the ISP Roadmap. |
Stretch into discomfort and keep doing it. |
| Many revolutions lock in new normal at each incremental permanent change in flexion. | Once-and-done, no repetitive motion. |
Bottom line
When your knee mobility is at stake, you do not have to settle for therapy as narrowly focused as static stretching. Braces and splints
• will not be part of your life going forward
• do not push you toward a lifetime of functional movement, and
• are so much less fun than cycling.
Moving beats sitting. You have an alternative.
I invite you to experience rehabbing your arthrofibrotic knee with OrthoBike: multi-dimensional and forward-looking.
Contact us to learn more about OrthoBike HERO or to reserve one for home use →
Click here for a technical review of the science behind OrthoBike.
Nothing in these posts is intended as medical advice or as a guarantee of any level or kind of outcome. The science of cycling in therapy and high- and low-intensity stretching is established. The physiological and psychological conditions of people vary. Consult with your medical care team.
Archimedes of Syracuse and Knee Rehab
I want to share a family story with you.
My Greek ancestors tell the story–all oral history, so of course it’s got to be true–that our cousin, Archimedes of Syracuse, also exclaimed “Eureka” when he realized he could rehab his arthrofibrotic knee by cycling with a 2-inch pedal crank.
He had done the math and leg measurements as only he could and realized to his profound relief that the length of the pedal crank and seat position determined his maximum pedaling knee flexion.
The story unfortunately ends before he regained his full range of motion.
Archimedes was pedaling and contemplating the deeper mechanics of knee rehab when the Romans attacked, which wasn’t nearly as great a concern to him as his knee. He refused to give up his novel device to a Roman soldier, whose knee was also quite stiff and painful, when the soldier demanded it at the point of his gladius.